







Lightning strikes between clouds and ground objects occur when the difference in electrical potential between the two is greater than 30,000 Volts, as thus they are able to exceed the atmospheric electrical resistance, generating currents that vary from 30,000 to 100,000 Amperes, and lasting between 0.1–0.001 seconds. As per data from the Lightning Imaging Sensor (LIS)-equipped satellite developed by the National Aerospace Agency (NASA), globally it is estimated that 44 flashes occur per second, with 1.4 billion flashes occurring in a year.1,2
Thunderstorms with associated lightning occur in all parts of the UK throughout the year, with the highest incidence in the southeastern part of England between May and August.3,4 According to the Tornado and Storm Research Organisation (TORRO), in a typical year between 200,000 and 300,000 lightning counts take place, and of these approximately one in four will provide a cloud-to-ground electrical discharge.
Twenty-four thousand people are thought to die from lightning-related injuries every year around the world.5 The yearly worldwide death rates from lightning range from 0.2 to 1.7 per million population.6 In the UK between 1988 and 2012, the TORRO database has recorded 445 incidents involving 722 people, with an annual average of two fatalities and 30 injured victims per year, and hospital coding records show that 63 patients were treated in an in-patient or out-patient setting due to lighting-related pathologies.7 In one third of the recorded incidents, more than one person was involved. Half of the recorded incidents occurred indoors and these were non-fatal, though the majority of people suffered a strike when they were involved in outdoor activities.7
The electrical current may reach the body in several ways, both directly and indirectly and this has been well reviewed by Elsom and Webb.7 In a direct strike which commonly involves the upper extremities, the current passes over the surface of the body, without most of it penetrating the victim (‘external flashover’). Depending on the amount and duration of current penetration, injuries may vary from simple erythema to serious multi-organ injury and cardio-pulmonary arrest. Indirect mechanisms of injury involve the victim making contact with an electrified object or the ground, which act as conductors for a nearby lightning strike, and these mechanisms are mainly responsible for indoor injuries. Apart from the direct effects of electricity, victims may also suffer injuries from blunt trauma due to explosive air expansion and pressure waves, get caught in nearby fires, or wounded by falling objects or projectiles.7
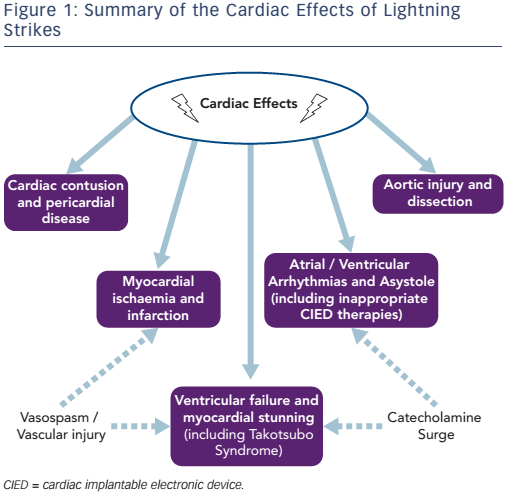
Almost every organ system can be involved in lightning strikes, and prognosis depends on systemic effects. There are similarities with domestic and industrial electric shock accidents and reported pathology includes skin changes (including the characteristic fern-like or Lichtenberg figure erythema), localised and deep burns, severe muscle contractions with paralysis and necrosis, central and peripheral nervous system injuries, secondary multi-organ failure as well as cardiovascular effects. The latter are the focus of this review (Figure 1) as they are very common and one of the main modes leading to death in these victims.8–10 The physical injuries may resolve completely or may be associated with long-term effects, including psychological sequelae for the survivors.11
Cardiac Effects of Lightning Injury
Arrhythmias
The huge rise in voltage accompanying lightning strikes can result in a massive direct current shock, which in turn is capable of depolarising the entire myocardium.9,12 Furthermore, increased autonomic stimulation as a result of the shock received, with an associated catecholaminergic surge have additive effects on the heart rate and rhythm.13,14
It has been thought initially that electrically-induced asystole was the commonest presenting rhythm; hence by proceeding and resuscitating these victims, there was a good chance of a successful outcome.15–17 However, subsequent research has shown that ventricular arrhythmias, including ventricular tachycardia (VT) and fibrillation (VF), are much more common than initially thought.16,18 In a large case series by Wetli and colleagues, ventricular arrhythmias have been reported by paramedics arriving on site, as the first recorded rhythm in at least 50 % of the victims whose electrocardiographic (ECG) data were available.18 Specifically, out of 20 victims VF was recorded in 10 patients, idioventricular rhythm in one, pulseless electrical activity (PEA) in one and asystole in eight patients.18 It is also important to note that asystole may be perpetuated, or be secondary to medullary dysfunction.19
Less sinister arrhythmias such as atrial fibrillation have also been reported, which can readily cardiovert to sinus rhythm in the ensuing days, especially with beta-blocker therapy.20–22
Other important ECG changes which have not been linked with any arrhythmias include QT prolongation, likely due to repolarisation abnormalities. Several mechanisms can be attributed to this, including alterations in intracellular calcium .23 McIntyre and colleagues reported QTc prolongation to 500 ms in a lighting victim which developed 2 days after the index event, whereas in a patient reported by Palmer et al. , the QTc prolonged to 680 ms, and normalised after 1 month, hence the potential need for initial and long-term ECG follow-up of these patients.23,24
Finally, with regards to management of these patients in the immediate setting, even though asystole or PEA are traditionally associated with worse prognosis, as the majority of the victims of lightning strikes tend to be young with no underlying comorbidities, prolonged resuscitation can lead to successful outcomes.25,26
Cardiac Implantable Electronic Devices
Though the passage of electric current typically does not damage or reprogram the cardiac implantable electronic devices (CIEDs), device therapy can be inadvertently affected if the degree of electromagnetic interference (EMI) is significant enough to overcome the electric insulation. Metallic objects of different sizes carried by victims, such as bra fasteners and safety pins have been reported to acquire magnetic properties in lightning victims.18 Furthermore, transient intense magnetic fields have also been documented to develop in the surrounding environment of a lightning strike.27 The above raise the theoretical risk of proxy sources for EMI if found close to the device pocket.
There have been several case reports for electrocution victims in whom their CIED delivered an appropriate therapy. Ginwalla et al. described the case of an electrocuted patient saved by their Implantable Cardioverter Defibrillator (ICD), which was able to pace asynchronous when needed with initiation of their noise reversion mode, and defibrillate successfully a ventricular arrhythmia following resolution of the surrounding EMI.28 Similarly, electrocution victims have also been successfully defibrillated by their ICD, as reported by Perret and Lappegård.29,30 Nonetheless, EMI from electrical equipment, commonly due to current leakage, while usually not enough to result in electrocution, is well known to result in inappropriate device therapies.31–33
However, the literature is scarce with regards to the effects of lightning strike and CIEDs. Only a couple of case reports exist with both appropriate and inappropriate shocks documented. Anderson and colleagues reported an inappropriate ICD shock in a patient who was in a shower house that was hit by a lightning. Subsequent device interrogation has shown multiple episodes of interference after the lightning strike, which briefly rose significantly in amplitude for the device to erroneously detect this as VF and deliver an inappropriate shock.34 Interestingly, the original shock received by the patient during the strike was also detected by the device. In contrast, Kondur and colleagues reported on the case of a 75-year-old patient who was successfully defibrillated by his ICD, following electrocution by a lightning strike.35 There is no sufficient data that look at the long term impact of lightning on the hardware such as the leads and their connection points. Though metallic objects carried by patients such as coins and zip fasteners have been found to be fused and morphologically altered, there are no reports of any internal destruction of CIED components.18
Myocardial Infarction
ECG changes suggestive of myocardial ischaemia have been widely reported in the literature for some time.16,36,37 These include ST segment elevation and depression, as well as widespread T wave inversions. Furthermore, there is scarce evidence that there may be a correlation of localising ischaemic ECG changes with myocardial injury on autopsy specimens.13,38 Tachyarrhythmias described above may also have a secondary adverse effect by starving the myocardium of oxygen.
Nonetheless some controversy still exists as to whether these can correlate fully with underlying pathological evidence of myocardial necrosis due to coronary-mediated ischaemia. Cardiac enzymes have been reported either as being elevated or within normal limits in patients who had ECG changes suggestive of cardiac ischaemia.24,39 This is not surprising as several mechanisms may have an impact on the levels of biochemical markers apart from coronary ischaemia, including cardiac contusion (which is reviewed below), tachyarrhythmias, acute kidney injury, leakage from skeletal muscle as well as the resuscitation process itself.
On a macroscopic level, coronary vasospasm as well as thrombotic occlusions have been proposed as the underlying mechanisms leading to a reduction in coronary blood flow.24 Transient coronary vasospasm may explain to an important extent why in patients with ST segment changes, their immediate coronary angiography results show patent vessels with no signs of stenosis – a finding also seen in electrocution victims.40–44 Looking closely at these cases, in several patients the ST segment changes followed defibrillation for malignant arrhythmias, which raises the prospect that these may also represent persistent repolarisation changes due to cellular injury, which may spontaneously resolve if left enough time. Furthermore, these changes are seen in previously healthy children struck by lightning, making the prospect of coronary lesions unlikely.41 Microscopically, in several cases myocardial infarction has been established in histological cardiac examinations of the victims, with features of possible thrombotic infarction such as endothelial damage and coagulation necrosis.13,38,40
Further studies are required to better correlate myocardial ischaemia as a direct effect of persistent coronary occlusion in these victims and thus identify those who would benefit from immediate coronary interventions after resuscitation.
Myocardial Contusion, Pericardial Disease and Aortic Injury
Cardiac contusion is an important mode of mortality and morbidity in children and adult victims. Even though this can lead to instant death, victims have also been reported to succumb to this type of injury days after the index event.18 In autopsy studies, haemorrhagic spots have been identified in areas not associated with large coronary vessels, as well as tracking along large unobstructed tributaries to the coronary tree. These areas can span the whole of the myocardium wall, from subendocardial to epicardial regions and there is often an associated myocardial tearing and haemopericadium with tamponade.18 The mechanisms of injury can either be related to the direct effect of current passage or secondary effects due to explosive environmental effects and blunt trauma. Depending on the extent of myocardial damage and degree of cardiac stunning, patients may develop cardiogenic shock which can be reversed with supportive measures.24 Elevations in cardiac enzymes including troponin and creatine kinase have been reported; however, the prognostic significance has yet to be determined.40 Cardiac contusion should thus be suspected in all victims who present with cardiovascular compromise and have features of impaired contractility and relaxation on their cardiac imaging.
Close cardiovascular monitoring can also detect early on pericardial collections which apart from contusion, may also accompany pericarditis which may be the result of myocardial inflammation and necrosis. Pericardial effusions have been reported to develop and persist in the first 2 weeks, and in rare cases pericarditis can reoccur for several months after the event.40
Finally, reference should be made to aortic trauma, as separation of the medial and intimal layers or medial defects, ultimately leading to fatal dissections, has also been well described.18 The mechanisms of these are likely to be similar to the ones causing cardiac contusion and the two pathologies can potentially co-exist.
Ventricular Failure and Myocardial Stunning
As described in the previous section, patients may develop cardiovascular compromise and ventricular failure due to a host of aetiologies including arrhythmias, cardiac ischaemia and myocardial necrosis. These mechanisms, and specifically catecholamine-mediated cardiotoxicity or ischaemia due to coronary vasospasm associated with lighting strikes, may also explain the finding of Takotsubo Syndrome with apical ballooning, included in several case reports of both young and older victims.45 In 2005, Hayashi and colleagues reported the first case of a 62-year-old mountaineer, who was struck by lightning and her echocardiography was suggestive of a takotsubo-like pattern of left ventricular hypokinesis. This resolved after 48 hours.46 Though transient, this condition should not be underestimated as Dundon et al. described the case of a younger female who developed more significant complications with cardiogenic shock following lightning-induced takotsubo cardiomyopathy.47 In the latter case, the patient’s cardiac function returned to normal after 6 weeks. Interestingly, in both of these cases the victims were female, which correlates with the overall gender bias of this condition, as nine out of 10 patients tend to be female.45
Though not commenting on the pattern of left ventricular dysfunction, Rivera and colleagues described a similar case of rapid deterioration of a 42-year-old, female lightning victim, who developed cardiogenic shock requiring inotropic support, attributed to myocardial stunning. Similar to the cases above, her condition improved, and 9 days after the index event, she made a complete recovery with full restoration of her cardiac function.48 Levosimendan, a calcium sensitiser, was used as the inotropic agent, and given the patient’s response, the authors pondered whether disturbances in calcium metabolism as well as reduced calcium sensitivity of myofilaments may play a key role in this situation.48 No inotropic support was required in the patients reported by Dundon and Hayashi above.46,47
Protective Measures for Exposed Individuals During Lightning Storms
Lightning strikes can have devastating effects, with significant cardiac and non-cardiac complications. Over the last three decades, there has been a reduction in the case fatality rate.7,49,50 This can be attributed to several reasons including better public education and safety regulations for outdoor and indoor activities, lightning protection measures in buildings and other structures, as well as medical pathways and protocols to promptly tend to and manage victims effectively.7 Nonetheless, despite ease of access to more accurate weather forecasting and thunderstorm warning systems, people may still get caught in adverse weather. Key precautionary measures to limit the risk of potential injury during a lightning strike are summarised below.
Outdoor Exposure
Any person who is caught in a thunderstorm while engaging in outdoor activity in an exposed terrain such as a hill or the seaside, should promptly seek an appropriate shelter. Promptly exit and avoid any body of water where the body will act as a peak or ‘beacon’ for a potential strike. Seek a well-grounded, enclosed building, or if this is not available an enclosed metal-topped vehicle (which will dissipate the electric current around the victim and directly to the .7 Hiding under trees can be a lethal decision as electric current from a potential tree strike can conduct to the victim from the trunk, or significantly injure the person from explosive decompression of vaporized sap.51 Furthermore, following a strike, it is important to avoid touching objects or building structures which are insulated from the ground, as they may retain electrical charge for some time.7 However, this does not apply to the body of a victim, and if cardiopulmonary resuscitation is required, including defibrillation, this should be initiated promptly.
Carrying or wearing small metallic objects such as keys or necklaces will not make a person more prone to be struck, but these can cause substantial localized burns or conduct an electrical current to deeper body structures, such as in the case of earphones or mobile phones and inner skull injuries.7
Indoor Exposure
Apart from the rare risk of lightning entering the building through an opening such as a door or window, most indoor victims receive an electrical charge through indirect means involving electrical wiring or plumbing which conduct electricity from a nearby strike. Common culprits to be avoided are corded phones, computers which are plugged to the electrical mains and radiators.50,51
Lightning protection systems incorporating lighting conductors or rods, the concept of which was originally described by Benjamin Franklin, protect structures and their occupants during electrical storms.52 These are made from highly conducting materials such as copper or aluminum, and when they are struck by lightning, they provide a low-resistance path and hence preferential route for the electrical current to travel from the top of the building to the ground, and away from the structure they protect. In the UK, there has been a substantial decrease over the last 30 years in the number of indoor fatalities compared to previous decades, which can be attributed to a combination of better lightning protection systems and effective grounding, as well as enclosing exposed wiring and plumbing in walls.7,49,50
Conclusions
Cardiac effects of lightning strikes are an important mode of morbidity and mortality; these include benign and life-threatening arrhythmias, inappropriate therapies from cardiac implantable electronic devices, cardiac ischaemia, myocardial and aortic injury as well as cardiomyopathy with associated ventricular failure. Further research is required to identify prognostic markers, either with regards to the patient’s biochemistry or cardiac imaging results, in the acute setting in the ‘stable’ patient, thus establishing which ones may likely develop more sinister complications later on, as well as those who will benefit from close rhythm monitoring on discharge. Finally, as the association between electrocardiographic ischaemic changes and underlying coronary obstruction is not fully established, further studies are required in this area to identify which patients require to be rushed to the cath lab at an early stage, thus avoiding unnecessary invasive procedures.